Obstructive Sleep Apnea: Symptoms, Causes & Treatment Treatment & Prevention
Are you waking up gasping for air at 3 AM? Does your partner complain that you sound like you stop breathing during the night? You’re not alone. An estimated 22 million Americans have obstructive sleep apnea (OSA), yet nearly 80% remain undiagnosed. This sleep-breathing disorder doesn’t just steal your rest—it can quietly damage your heart, increase your stroke risk, and tank your daytime productivity without you even realizing what’s happening.
The frustrating part? Many people dismiss their symptoms as normal snoring or attribute their exhaustion to stress. But sleep apnea is different. It’s a serious condition where your airway repeatedly collapses during sleep, cutting off oxygen to your brain and forcing your body into a fight-or-flight response dozens—sometimes hundreds—of times each night. The good news is that OSA is highly treatable, and you don’t have to live with the constant fatigue and health risks anymore.
In this comprehensive guide, we’ll walk you through everything you need to know about obstructive sleep apnea: what causes it, how to recognize the warning signs, why diagnosis matters, and the treatment options that actually work. Whether you suspect you have sleep apnea or you’ve already been diagnosed, you’ll find practical, actionable insights to help you reclaim better sleep and better health.
What Is Obstructive Sleep Apnea, Really?
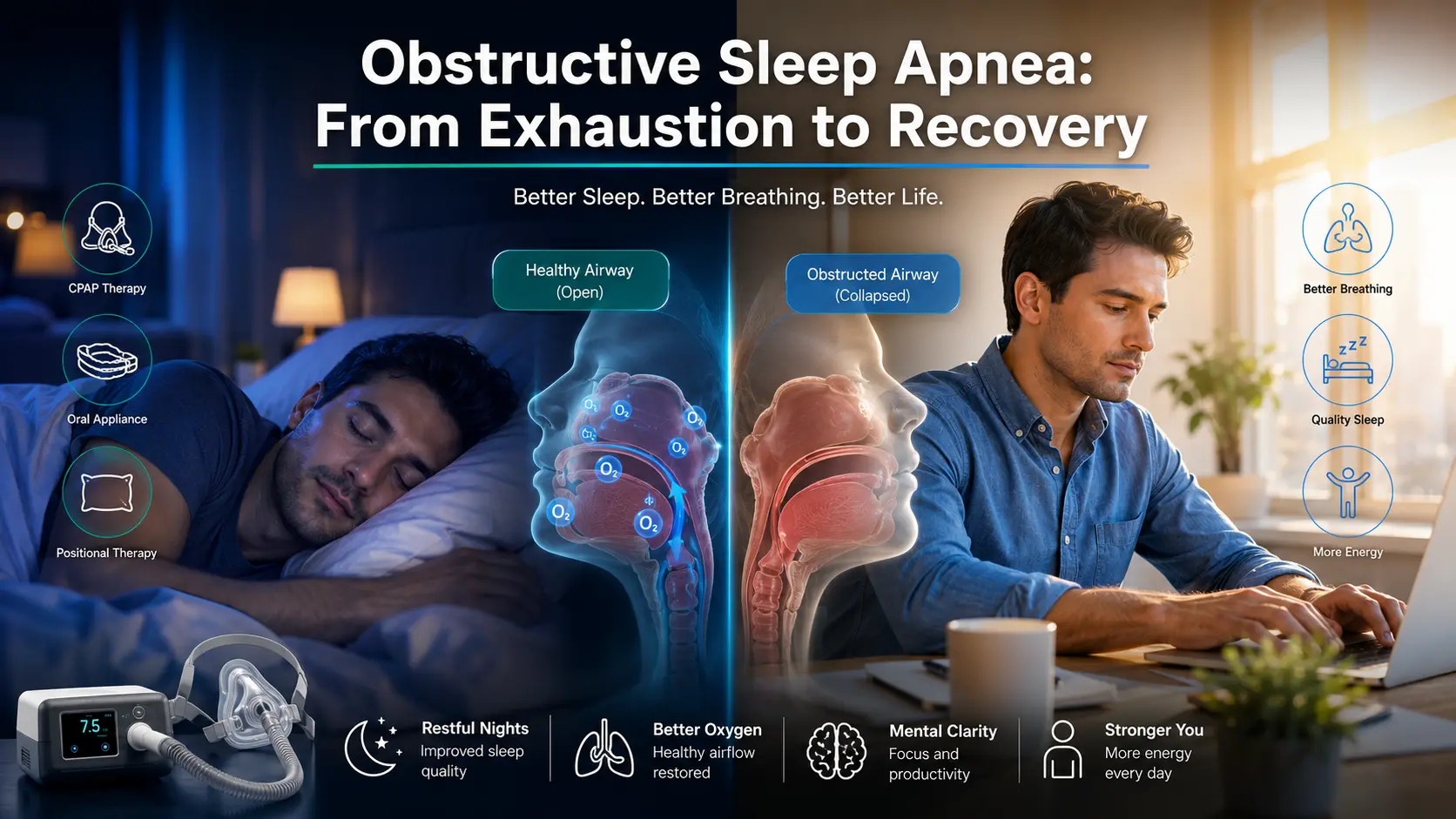
Let’s start with the basics. Obstructive sleep apnea happens when the muscles at the back of your throat relax excessively during sleep, causing your airway to narrow or collapse completely. When your airway narrows, airflow to your lungs decreases, which is called a “hypopnea.” When it closes entirely, it’s called an “apnea.” This happens because your brain senses the drop in oxygen levels and briefly awakens you to reopen your airway—often with a loud gasp or snort.
Here’s where it gets problematic: these micro-awakenings are so brief that you often don’t remember them, but they fragment your sleep architecture and prevent you from reaching deep, restorative sleep stages. Someone with moderate to severe OSA might experience 30, 50, or even 100+ of these events every hour.
The severity of OSA is measured by the Apnea-Hypopnea Index (AHI):
- Mild OSA: 5-14 events per hour
- Moderate OSA: 15-29 events per hour
- Severe OSA: 30+ events per hour
Think of it this way: during a normal night of sleep, you should have fewer than 5 breathing events per hour. If you’re experiencing 40+ events per hour, your airway is being obstructed multiple times per minute. That’s not just affecting your sleep quality—it’s creating cumulative stress on your cardiovascular system.
Recognizing the Symptoms: What to Watch For
OSA symptoms fall into two categories: what happens at night and what you experience during the day. The tricky part is that many people experience symptoms without realizing they’re connected to a breathing disorder.
Nighttime Symptoms (What Your Partner Might Notice First)
- Loud snoring that disrupts your partner’s sleep (sometimes described as gasping, choking, or grunting sounds)
- Observed breathing pauses during sleep (your partner notices you stop breathing, then gasp suddenly)
- Restless sleep with frequent position changes and tossing
- Night sweats unrelated to room temperature or bedding
- Nocturia (waking multiple times to urinate, which isn’t normal)
- Teeth grinding (a stress response to repeated arousals)
Daytime Symptoms (What You’ll Notice)
- Excessive daytime sleepiness (EDS) even after a full night’s sleep—that bone-deep fatigue that makes you feel like you’re operating with a mental fog
- Morning headaches that persist even after coffee
- Difficulty concentrating at work or while driving
- Memory problems and brain fog
- Mood changes including irritability, anxiety, or depression
- Reduced sex drive (a symptom many don’t connect to OSA)
The severity of daytime symptoms doesn’t always correlate with AHI scores. Someone with mild OSA might feel profoundly exhausted, while someone with severe OSA might not notice daytime symptoms initially. This is why self-reporting matters—your experience is valid regardless of what the numbers say.
OSA Across Different Demographics
In Children: Parents often misintribute OSA symptoms to ADHD. Watch for poor school performance, behavioral problems, pauses in breathing during sleep, and sometimes failure to grow normally.
In Women: Sleep apnea was historically underdiagnosed in women because the classic presentation (loud snoring) is less common. Women are more likely to report fatigue, insomnia, mood disturbances, and morning headaches. If you’re a woman and your sleep apnea screening came back negative, but you still feel exhausted, ask about positional OSA or less typical presentations.
In Older Adults: Symptoms might be subtler—confusion, falls, or worsening hypertension rather than obvious daytime sleepiness.
What Actually Causes Obstructive Sleep Apnea?
OSA isn’t caused by a single factor. Instead, it’s the result of multiple interconnected factors that vary from person to person. Understanding your specific risk factors is important because it influences your treatment approach.
Anatomical Factors (The Structure of Your Airways)
Your airway is naturally narrower when you’re lying down, which is why gravity plays a role. Some people have:
- Naturally smaller airways due to their genetic makeup
- Enlarged tonsils or adenoids that physically block airflow
- A deviated septum that restricts nasal airflow
- A longer soft palate or uvula that’s prone to collapse
- A larger tongue (macroglossia) that takes up more space in the throat
- A recessed chin (micrognathia) or overbite that changes airway geometry
The important distinction: If OSA were purely anatomical, everyone with small airways would have sleep apnea. They don’t. This tells us that anatomy is a vulnerability, not destiny.
Lifestyle and Weight Factors
Excess weight is the most modifiable risk factor for OSA. Even a 10% weight gain can worsen existing apnea; conversely, a 10% weight loss can improve it significantly. Fat deposits around the neck and throat constrict the airway, and excess visceral fat affects breathing mechanics.
But here’s the nuance: not everyone with sleep apnea is overweight, and not everyone who’s overweight has sleep apnea. Weight amplifies risk but doesn’t cause it independently.
Other lifestyle factors include:
- Sleeping on your back (positional OSA often improves dramatically when you sleep on your side)
- Alcohol consumption before bed (relaxes throat muscles and suppresses the arousal response)
- Sedative medications including sleep aids and anti-anxiety drugs
- Smoking which inflames airways
- Poor sleep hygiene that creates sleep fragmentation
Medical Conditions That Increase Risk
- Hypertension (high blood pressure)
- Type 2 diabetes
- Heart disease or atrial fibrillation
- Stroke history
- PCOS (Polycystic Ovary Syndrome) in women
- Hypothyroidism
- Acromegaly (hormonal disorder causing facial and throat enlargement)
- Nasal congestion or allergies that obstruct nasal airflow
Age, Sex, and Genetics
- Age: OSA prevalence increases significantly after age 40, though it can occur at any age
- Sex: Men are 2-4 times more likely to have OSA than women, though this gap narrows significantly after menopause when hormonal changes affect airway stability
- Family history: If your parent or sibling has OSA, your risk is elevated
The genetic component isn’t just about anatomy—it’s also about how your brain responds to airway collapse. Some people’s brains are hypersensitive to even small drops in oxygen (they arouse easily, preventing severe apneas but causing sleep fragmentation). Others have more delayed arousal responses (longer apneas but potentially better sleep continuity). Neither pattern is ideal; they just present differently.
The Serious Health Consequences of Untreated OSA
This is where OSA stops being merely an inconvenience and becomes a genuine health concern. Untreated obstructive sleep apnea doesn’t just affect your sleep quality—it systematically stresses your body’s most critical systems.
Cardiovascular Consequences
Each apneic event triggers a cascade: oxygen drops, your sympathetic nervous system activates, heart rate spikes, blood pressure surges. Repeat this 50 times per hour, night after night, and you can see why OSA dramatically increases cardiovascular risk:
- Hypertension: Up to 80% of people with resistant hypertension have undiagnosed OSA
- Atrial fibrillation: The irregular heartbeat that can lead to stroke
- Heart attack and stroke: The risk is 2-3 times higher in untreated OSA
- Heart failure: Both systolic and diastolic dysfunction can worsen with OSA
- Sudden cardiac death: Rare, but documented in severe untreated cases
Metabolic Effects
- Insulin resistance: The repeated oxygen deprivation impairs glucose metabolism
- Type 2 diabetes: OSA increases risk and complicates blood sugar control
- Weight gain: Sleep fragmentation alters hunger hormones, increasing appetite and cravings
- Elevated cholesterol: Particularly triglycerides
It’s a vicious cycle: OSA contributes to weight gain, weight gain worsens OSA. This is why weight loss alone often isn’t the complete solution—you need to address the breathing disorder directly.
Cognitive and Mental Health Impacts
- Memory problems: Both short-term recall and long-term memory suffer
- Attention deficits: Concentration becomes difficult, affecting work performance
- Executive function decline: Decision-making and planning suffer
- Mood disorders: Depression and anxiety are significantly more common
- ADHD-like symptoms: Particularly in children, OSA is sometimes misdiagnosed as ADHD
Safety and Accident Risks
People with untreated OSA are involved in motor vehicle accidents at rates 5-7 times higher than the general population. The excessive daytime sleepiness isn’t just uncomfortable—it’s genuinely dangerous.
How Obstructive Sleep Apnea Is Diagnosed
Diagnosis requires more than just recognizing symptoms. You need a formal sleep study to confirm OSA, measure its severity, and rule out other sleep disorders.
Step 1: Initial Screening
Start with your primary care physician or a sleep medicine specialist. They’ll ask about:
- Your sleep and daytime symptoms
- Risk factors (weight, age, medical history)
- Your family history
- Medication list (some meds worsen sleep apnea)
Simple screening questionnaires like the STOP-BANG scale or Epworth Sleepiness Scale can flag patients for further testing, though these aren’t diagnostic.
STOP-BANG questions:
- Do you Snore loudly?
- Do you experience daytime sleepiness or doze off?
- Has anyone observed you Stop breathing during sleep?
- Do you have high blood Pressure?
- Is your BMI over 35?
- Is your Age over 50?
- Is your Neck circumference over 40 cm (about 16 inches)?
- Is your Gender male?
A score of 3+ suggests you should pursue sleep testing. Even lower scores don’t rule out OSA, particularly in women and younger patients.
Step 2: Sleep Study Options
In-Lab Polysomnography (PSG): The gold standard. You spend a night at a sleep center connected to equipment that monitors:
- Brain activity (EEG)
- Eye movement (EOG)
- Muscle activity (EMG)
- Heart rhythm (ECG)
- Oxygen saturation
- Airflow
- Chest and abdominal movement
- Leg movements
- Body position
A technician watches throughout the night (they’re not judging your sleep habits—they’re data collecting). Cost: typically $1,500-$3,000, though insurance usually covers it.
Home Sleep Apnea Test (HSAT): A portable version that measures airflow, oxygen levels, heart rate, and breathing effort. You take the device home, sleep normally, and return it the next day. This is increasingly popular because it’s:
- More convenient
- Less expensive ($300-$600)
- Often covered by insurance
The limitation: HSAT can’t detect central sleep apnea or other sleep disorders. If HSAT results are inconclusive or if central sleep apnea is suspected, you’ll need lab testing.
Step 3: Understanding Your Sleep Study Results
Your results will include an Apnea-Hypopnea Index (AHI) score:
- AHI < 5: Normal (no sleep apnea)
- AHI 5-14: Mild OSA
- AHI 15-29: Moderate OSA
- AHI 30+: Severe OSA
You’ll also see your oxygen saturation levels (how low your oxygen drops during events), the arousal index (how many times your sleep is disrupted), and notes on any position-dependent patterns.
What this means: A patient with AHI of 25 is having roughly 25 breathing interruptions per hour. If they sleep 7 hours (420 minutes), they’re experiencing approximately 175 complete airway closures during that night.
Comprehensive Treatment Options for OSA
The good news: OSA is highly treatable. The challenge is finding the approach that works for your specific situation and that you’ll actually stick with consistently.
CPAP Therapy (Continuous Positive Airway Pressure)
CPAP is the most commonly prescribed treatment. A small machine delivers pressurized air through a mask that keeps your airway open throughout the night. It’s remarkably effective—when used properly, CPAP normalizes oxygen levels and virtually eliminates apneic events.
Why people abandon CPAP:
- Mask discomfort or claustrophobia
- Difficulty adjusting to the sensation
- Noise (though modern machines are quieter)
- Nasal congestion from the air pressure
- Inconvenience while traveling
How to succeed with CPAP:
- Start with a gradual acclimatization program (wearing it during the day while watching TV)
- Experiment with different mask styles and sizes—comfort matters
- Use a heated humidifier to prevent dryness
- Work with your sleep center’s CPAP coordinator; they can adjust settings
- Give yourself 2-3 weeks of consistent use before deciding it’s not working
- Connect with CPAP support communities—you’re not alone in this adjustment
Cost: $400-$1,500 for the machine; $30-$100/month for supplies with insurance coverage varying widely.
BiPAP and AutoPAP Alternatives
- BiPAP (Bilevel Positive Airway Pressure): Delivers two different pressure levels—higher when you inhale, lower when you exhale. Some people find this more comfortable than CPAP.
- AutoPAP: Automatically adjusts pressure throughout the night based on your breathing patterns, which some patients prefer.
Oral Appliances (Mandibular Advancement Devices)
These mouthpiece-like devices physically move your lower jaw forward slightly, which opens the airway. They’re particularly effective for mild to moderate OSA and are excellent for people who:
- Can’t tolerate CPAP
- Travel frequently
- Have position-dependent OSA (since they work regardless of sleeping position)
Considerations:
- Must be custom-fitted by a dentist trained in dental sleep medicine
- Requires ongoing dental monitoring
- Works best if you have sufficient teeth
- Can cause jaw joint discomfort initially
- Generally effective for mild to moderate cases; less effective for severe OSA
Cost: $1,500-$3,000 initially, often with insurance coverage.
Surgical Options
Surgery is typically considered when other treatments fail or aren’t feasible:
- Uvulopalatopharyngoplasty (UPPP): Removes excess soft palate and uvula tissue. Success rates vary (40-60%), and symptoms can return over time.
- Genioglossus advancement: Moves the attachment point of the tongue muscle forward to prevent collapse.
- Septoplasty: Corrects a deviated nasal septum to improve airflow.
- Palatal implants: Stiffens the soft palate with small implants.
- Maxillomandibular advancement: Moves the upper and lower jaw forward (most invasive but can be highly effective for severe cases).
Surgery works best when there’s identifiable anatomical obstruction, but it’s not a universal solution. Success depends on where in your airway the collapse is occurring.
Positional Therapy
For positional OSA (symptoms that worsen or only occur when sleeping on your back), positional therapy can be remarkably effective:
- Sleep on your side (side-sleepers have fewer apneic events)
- Use positional sleep devices that vibrate if you roll onto your back
- Specialized pillows that encourage side sleeping
- Even taping a tennis ball to the back of your pajamas as a DIY solution
This works because gravity’s effect on airway collapse decreases dramatically when you’re not lying flat on your back.
Lifestyle Modifications
These work best combined with other treatments, not as a standalone solution:
- Weight loss: A 10% reduction often meaningfully improves OSA
- Exercise: Beyond weight loss, cardiovascular exercise improves oxygen utilization
- Avoid alcohol: Especially 3+ hours before bed
- Avoid sedating medications: When possible, discuss alternatives with your doctor
- Treat allergies: Nasal congestion worsens OSA
- Sleep position: Back sleeping is the worst position for OSA
- Quit smoking: It inflames airways
- Sleep hygiene: Consistent bedtimes, dark cool rooms, etc.
Prevention and Long-Term Management
Once diagnosed, OSA is lifelong management, not a condition you “cure” and move on from. Your focus shifts to preventing progression and maintaining treatment compliance.
Weight Management as Prevention
If you don’t have OSA yet but have risk factors, weight management is genuinely protective. Even modest weight loss (5-10%) can delay or prevent OSA onset. This is particularly important if you have:
- A family history of sleep apnea
- Hypertension or metabolic syndrome
- PCOS (in women)
- Early signs of sleep-disordered breathing
Nasal Health Optimization
Your nasal airway is the first line of defense. Poor nasal airflow forces you to breathe through your mouth, destabilizing your throat and worsening apnea. If you have:
- Allergies: treat aggressively (nasal sprays, antihistamines, consider immunotherapy)
- Deviated septum: consider septoplasty
- Chronic sinusitis: get appropriate treatment
- Nasal polyps: these can be surgically removed
Even simple measures like saline rinses before bed can help.
Regular Sleep Specialist Follow-Up
You’re not done after initial diagnosis. Annual (or bi-annual) follow-ups help:
- Assess how well your current treatment works
- Detect any progression or changes
- Adjust treatment as needed
- Screen for new symptoms
Screening for Comorbidities
Because OSA increases cardiovascular risk, your doctor should:
- Monitor blood pressure consistently
- Check for atrial fibrillation
- Assess heart function if indicated
- Monitor glucose levels
- Adjust medications for hypertension or other conditions based on OSA diagnosis
Common Mistakes People Make With Sleep Apnea
Mistake #1: Delaying Diagnosis
“I’ll just live with the snoring” or “I’m not that tired” often means years of undiagnosed OSA damaging your cardiovascular system silently. The sooner you know, the sooner you can prevent serious complications.
Mistake #2: Giving Up on CPAP Too Quickly
Many people use CPAP for 2-3 weeks, feel like it’s not working, and abandon it. The adjustment period is real—your body needs time to adapt. Most people report significantly improved sleep quality and daytime function after 4-6 weeks of consistent use.
Mistake #3: Assuming Weight Loss Will Cure OSA
Weight loss helps—sometimes significantly. But even people of healthy weight can have OSA. Don’t delay other treatments waiting for weight loss to work.
Mistake #4: Ignoring Mild OSA
“It’s just mild” is not a reason to skip treatment. Mild OSA still stresses your cardiovascular system and affects your daytime function. Most sleep specialists recommend treating even mild OSA if you’re symptomatic.
Mistake #5: Not Addressing Comorbidities
If you have OSA and hypertension, diabetes, or heart disease, these conditions interact. Treating only the OSA or only the other condition is incomplete management.
Mistake #6: Inconsistent Treatment Use
CPAP works only when you use it. Wearing it three nights a week doesn’t provide the same benefits as seven nights. Consistency matters more than perfection.
Expert Tips for Optimizing OSA Treatment
Work With a Sleep Medicine Specialist
While your primary care doctor can coordinate care, a board-certified sleep medicine specialist brings specialized expertise. They understand nuanced situations like:
- Mask fit optimization
- Pressure setting adjustments
- When to try different devices
- Complex interactions with other conditions
Use CPAP Data Tracking
Modern CPAP machines track usage hours, pressure data, and events. Download this data during appointments so your doctor can see:
- Your actual pressure needs
- Whether your settings are correct
- If you’re experiencing residual events despite treatment
Connect With Support Communities
Online CPAP support groups (Reddit’s r/CPAP, CPAPTalk forums, local sleep groups) provide real-world solutions from people who’ve navigated the same challenges. “I couldn’t tolerate my current mask type, so I tried X and it changed everything” advice is invaluable.
Be Proactive About Adjustment
If something isn’t working, speak up immediately. Small mask adjustments, humidifier settings, or pressure modifications can make the difference between compliance and abandonment.
Frequently Asked Questions About Obstructive Sleep Apnea
Q: What’s the difference between obstructive sleep apnea and central sleep apnea?
A: Obstructive sleep apnea happens when your airway physically collapses despite your body’s effort to breathe. Central sleep apnea occurs when your brain doesn’t send proper signals to breathe. OSA accounts for about 90% of sleep apnea cases; central sleep apnea is less common and sometimes occurs with heart failure or certain neurological conditions. Mixed sleep apnea has features of both.
Q: Can I have sleep apnea without snoring?
A: Yes, absolutely. While loud snoring is the classic presentation, approximately 25-50% of people with sleep apnea don’t snore, particularly women. You might just experience excessive daytime sleepiness, morning headaches, or be completely unaware until your partner notices breathing pauses.
Q: Will my sleep apnea go away if I lose weight?
A: Weight loss can significantly improve or even resolve OSA, particularly if excess weight was the primary cause. However, even people of normal weight can have sleep apnea. Weight loss should be combined with other treatments, not used as a substitute. A 10% weight reduction often provides meaningful improvement; 15-20% might result in substantial remission.
Q: Are there natural remedies for sleep apnea?
A: Lifestyle modifications (weight loss, positional therapy, nasal health optimization, avoiding alcohol) can help, but they’re rarely sufficient as standalone treatments, especially for moderate to severe OSA. These should complement, not replace, medical treatment.
Q: How quickly will I feel better after starting CPAP?
A: Some people notice improved alertness within 1-2 weeks; others need 4-6 weeks. Your brain has likely been oxygen-deprived for months or years—it takes time to recover fully. Daytime sleepiness typically improves first, followed by cognitive function and mood improvements.
Q: Can children have obstructive sleep apnea?
A: Yes. It’s often underdiagnosed in children and may present as ADHD, behavioral problems, poor school performance, or bedwetting rather than obvious daytime sleepiness. Enlarged tonsils or adenoids are common causes. If you notice pauses in your child’s breathing during sleep or unexplained behavioral changes, ask your pediatrician about sleep evaluation.
Q: Is sleep apnea permanent?
A: The anatomical features that contribute to OSA (airway structure, soft palate length, etc.) are relatively permanent. However, the severity can improve with weight loss, positional therapy, or treatment of contributing conditions. With proper management, OSA symptoms can be virtually eliminated.
Q: Will my insurance cover sleep studies and treatment?
A: Most insurance plans cover sleep studies and CPAP/BiPAP machines if OSA is diagnosed. Coverage varies for oral appliances and surgery. Ask your insurance company specifically or work with your sleep center’s billing department to understand your coverage before testing.
Q: What if I’m not compliant with CPAP?
A: Compliance is common, and there are solutions. If you’re struggling, talk to your sleep center before giving up. Different mask styles, machines, or settings might work better. Oral appliances or positional therapy might be alternatives. The key is finding a treatment you’ll actually use consistently.
Q: Can sleep apnea cause sudden death?
A: Sudden cardiac death is rare but documented in severe untreated OSA, typically in people with underlying heart disease. This is another reason why treating even mild OSA is important—it reduces cardiovascular risk.
Key Takeaways: Your Action Steps
- Recognize the symptoms: If you experience loud snoring, breathing pauses, excessive daytime sleepiness, or morning headaches, discuss sleep apnea screening with your doctor.
- Take screening seriously: Use the STOP-BANG questionnaire and don’t dismiss positive results. Sleep studies are non-invasive and invaluable.
- Understand your treatment options: CPAP is most common, but oral appliances, positional therapy, and lifestyle changes are legitimate alternatives. Work with your sleep specialist to find what works for you.
- Commit to consistency: Whether you choose CPAP, an oral appliance, or lifestyle modifications, consistent use matters far more than occasional compliance.
- Address underlying factors: Weight management, nasal health, alcohol avoidance, and sleep positioning all support your primary treatment.
- Monitor your progress: Use CPAP data tracking, schedule regular follow-ups, and report any changes in symptoms or concerns to your sleep specialist.
- Take cardiovascular health seriously: Since untreated OSA significantly increases stroke and heart attack risk, aggressive management of related conditions (hypertension, diabetes) is crucial.
- Don’t wait for “severe” symptoms: Mild and moderate OSA still deserve treatment if you’re symptomatic or at cardiovascular risk.
Conclusion
Obstructive sleep apnea is a serious condition, but it’s not a life sentence. With proper diagnosis and treatment, you can reclaim restorative sleep, eliminate daytime fatigue, and dramatically reduce your cardiovascular risk. The journey might require some adjustment—whether it’s adapting to a CPAP mask or committing to positional therapy—but the return to genuine, rested wakefulness is profoundly worth it.
You don’t have to feel exhausted every day. You don’t have to worry about your health in silence. You don’t have to let sleep apnea control your quality of life.
Start with one step: if you suspect you have sleep apnea, schedule an appointment with your primary care doctor and ask for a referral to sleep medicine. Take the screening questionnaires seriously. If recommended, pursue sleep testing without delay. Then, work collaboratively with your sleep specialist to find your optimal treatment pathway.
Your better sleep—and your better health—starts now.